New factsheets to help organisations and individuals meet the challenges of Covid-19
Professor Gail Kinman
CWH Director and Visiting Professor of Occupational Health Psychology, Birkbeck University of London
The Covid-19 pandemic has had a profound impact on the way that we live, and how and where we work. For many people it has been a time of setbacks and loss as businesses close, health is threatened, redundancy looms, and the effects of inequalities become ever more apparent. Although the economy seems to be recovering and we are gradually moving towards some degree of ‘normality’, the post-pandemic future is uncertain and little is yet known about its long-term implications for individuals and organisations. It is therefore crucial to support organisations and individuals in maintaining health and wellbeing during the pandemic and beyond and help policy makers meet the challenges they are facing.
Early in 2021, Public Health England commissioned the Society of Occupational Medicine (SOM) to organise a series of webinars and linked factsheets on the theme of ‘work, worklessness and wellbeing’. The project aimed to provide organisations and employees with practical guidance on key issues of concern during the pandemic. The project was guided by a steering group comprising leading experts and representatives from employers’ organisations. Along with the SOM, I organised these webinars and wrote the factsheets with input from the speakers and feedback from relevant bodies.
The webinars included high-profile speakers from organisations such as MIND, the Chartered Institute of Personnel and Development, Business in the Community, the British Psychological Society, the Health and Safety Executive, the Centre for Better Ageing and the Carnegie Trust. There were also presentations from leading academics in the field of work and wellbeing, business leaders and trade unions and professional associations. They were very well attended and feedback was overwhelmingly positive. Recordings of the webinars can be found here.
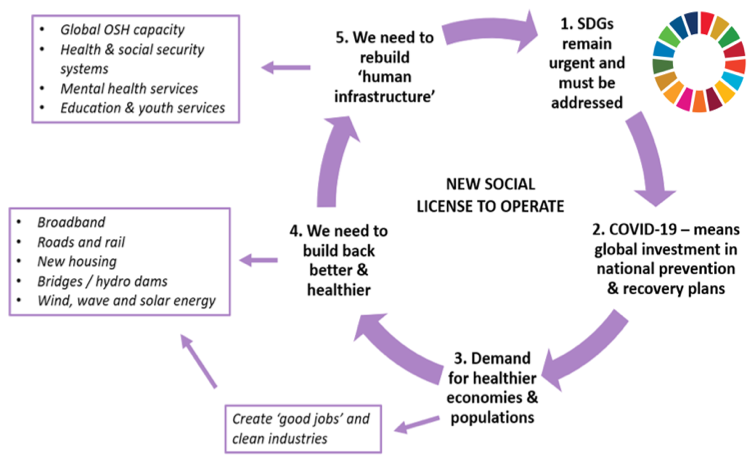
The factsheets have just been launched – each is informed by a review of research and provides a range of evidence-informed resources and tools to help organisations and individuals ‘build back better’. The topics addressed by the factsheets are shown below with links to download them:
- Supporting businesses to build back better: The benefits of age diversity
- Supporting your approach to workplace diversity and inclusion
- Creating better quality work and workplaces
- Managing stress, burnout and fatigue in health and social care
- Supporting workplace mental health and wellbeing during COVID-19 and beyond
- Developing a COVID-19 secure mental health and wellbeing strategy
- Managing change – restructuring, redundancy, and homeworking
Please disseminate the factsheets via your networks.